Understanding Complex Regional Pain Syndrome
Dedicated to providing knowledge for patients and healthcare providers.
Contact
Nancy is a disabled nurse with over 15 years helping others with CRPS. She has had CRPS herself since 1996.
About Nancy
I am Nancy Renée Cotterman. This is my CRPS/RSD (Complex Regional Pain Syndrome/Reflex Sympathetic Dystrophy) story.
In March of 1996, I was involved in an auto accident that resulted in 8 crush fractures of the metatarsals of my right foot. My foot absorbed all of the energy of the crash. At that time, I was working as a home care RN. Previously I had worked in Bryn Mawr Hospital as a pediatric nurse. I went to nursing school as an adult while working and raising my two young daughters. I worked so hard to become a RN.
The orthopedist ordered a CT of my foot (there were not MRIs back then). After he saw that the fractures were not displaced, he casted me in a non weight bearing cast for 8 weeks. At my next visit with the ortho, I told him that I was having burning pain and lightning like pain in my right foot. At a cast change, he noted that my foot was purplish blue. Unbeknownst to me, he charted my symptoms followed by, "I do not think that she has RSD (what CRPS was called then). A year later, the pain had intensified, my foot was still bluish purple and very swollen. The ortho felt that I had traumatic arthritis and recommended surgery to fuse the metatarsals of my right foot. That was followed by 8 more weeks of non weight bearing casting. After the surgery the pain was even more intense. I feel that my mistake about the surgery is that I should have gotten a second opinion. The orthopedist that I saw was a doctor that I had worked at at the hospital. He had repaired my mom's broken hip without complications and my daughter's broken wrist. After the surgery, I went to several other orthopedists for second, third and fourth opinions. They all said that my fusion had healed well. They were only looking at how well the surgery was healing, not at the whole picture of my symptoms. They all wait that there was no reason for my pain. In other words, it was all in my head.
I sank into deep depression. I attempted to take my life. Being told over and over that your pain is not real takes its toll. There is no relief because the medical profession think that it is all in your head. While I was in the hospital I was fortunate to be assigned to a psychiatrist who also worked at a rehabilitation hospital. He was the first one to tell me that my pain was not psychological; it was not all in my head. It was physical. He referred me to the director of pain at the rehabilitation hospital. He was a physiatrist (a doctor of rehabilitation medicine). He said, I think that you have RSD. He sent me for a three phase bone scan. (we now know that this is not a diagnostic test for CRPS). At our next visit he confirmed that I had RSD. I am a nurse. I had never heard of RSD. It is 1998 so there was no Google. I went onto my dial up internet and looked up RSD. What I read was not positive. One name came up over and over. That name was Robert Schwartzman. The name sounded familiar. I called my friend and asked her what her husband's boss' name was. It was Robert Schwartzman. I told my friend that the physiciatrist said that I had RSD. My friend told me that her husband had thought that I had RSD for a while. Why hadn't he mentioned that to me? Why did I have to hear over and over again that the pain was all in my head?
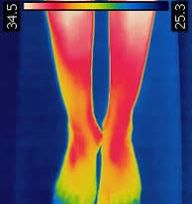
At that time, Dr Schwartzman (referred to as Dr S from now on) was not accepting new RSD patients. I was scheduled to see one of his co-workers, Dr LeBel. A thermo scan was done (measures the temperature changes in a limb compared to the other limb) and she confirmed that I had RSD.
I was actually relieved to finally have a physical diagnosis. It was the worst diagnosis I could have gotten. This was April 1998. At that time, the only treatments were sympathetic nerve blocks, spinal cord stimulators and intrathecal medication pumps. The first line of treatment was the sympathetic nerve block. They started with a bier block - a sympathetic nerve block of the foot. In the 1990's doctors felt that CRPS/RSD was a disorder of the sympathetic nervous system only. This is why it was named Reflex Sympathetic Dystrophy. We now know that CRPS affects the entire nervous system. The sympathetic nerve blocks makes sense if it was a defect of the sympathetic nervous system. After the block, my pain spread out of my foot and up my leg to the hip. An epidural nerve block was recommended. Following that block, the pain spread to the entire right side of my body. I refused any other blocks.
I was referred to a neurosurgeon. My pain flared up after I overdid it. That made it difficult to know when to stop and rest. The surgeon felt that for that reason, I was not a good candidate for a spinal cord stimulator. He suggested an intrathecal medication pump. We did a trial at the hospital and I had the surgery. My pump was filled with morphine. It really did not calm my pain. They upped and upped the dosage without success.
Shortly there after, my friend's husband called and told me that Dr S was doing a study of ketamine coma. Was I interested? I said yes. I met with Dr S. He felt that I was a good candidate. This was being done in Germany. The FDA would not allow the study in the U.S.
First, we had to wean me off the morphine. Opioids and ketamine compete for the same receptors. Dr S wanted the ketamine to attach to those receptors. To make a long story short, I went to Germany in October of 2001. I had been working up to this point. I stopped working in September 2001. Working helped my psychologically however I think that it was detrimental physically. I was 38 at the time of my accident. I could not imagine not working at that age.
I was the fifth American to get the ketamine coma therapy. When we went to Germany, we were sent by Dr S in pairs. The other person was also Nancy. She was a medical resident. I was never pain free. In addition to the CRPS nerve pain, I also had what I called my ortho pain that was not resolved by the fusion. The CRPS pain was gone for two months. It slowly started creeping back. The other Nancy was a surgical resident before her work related accident. She was able to get one of the anesthesiologists where she was a resident, to give us low dose ketamine as an outpatient in the hospital. He did the infusions in correlation with Dr S. They did not know what dosage would work or how frequently treatment would be needed. Once again, we both agreed to be test subjects. The dose was not high enough that I was out of it. I could read during the IV infusions. They tried having us come in Monday - Friday for two consecutive weeks for 4 hour infusions each day followed by a two week break. We did this for several months. I got moderate relief. Dr S began his own outpatient ketamine clinic. Because he was a neurologist rather than an anesthesiologist, Hahnemann capped the dosage of ketamine that he could administer. His protocol was considered low dose. He also established a protocol that involved a loading dose of ketamine for people new to ketamine and a booster protocol to boost the loading dose's effects.
By then, Dr S had gotten permission from the FDA and Hahnemann hospital to follow a protocol for inpatient ketamine that was being used by a doctor in Australia. I was admitted to the ICU for six days of continuous ketamine at 40 ml per hour. Again, I got relief but not the "cure" that Dr S had hoped for.
In 2012, Dr S announced that he was going to retire. By then, my husband and I had moved to FL. Through my blog, a pain management doctors nurse anethestisits contacted me. His physician and he were beginning a ketamine clinic for CRPS. They wanted to pick my brain. In December 2012, I began seeing Dr Ashraf Hanna for high dose ketamine infusions.
I remained depressed and on two antidepressants. I was 38 at the time of my accident. I had two daughters and a husband that depended on my. I was having difficult doing my daily activities. It was difficult not being able to work. The depression lessened when I found my niche. Dr S asked if I would be willing to speak to patients who were considering ketamine. Since I was a nurse, he felt that I could be factual and not overly emotional. That started my role as an advocate for CRPS. I also volunteered with a non-profit to be a mentor for those who were newly diagnosed. Once Facebook came along, I started a Facebook group to help others. Helping others, really helped me. It gave me a purpose especially when both of my girls were in college.
An added benefit was the recent acceptance of ketamine as an antidepressant. When I started seeing Dr Hanna for high dose, my psychiatrist suggested that we wean off my antidepressants. I was able to come off both of them while getting high dose ketamine infusions on a regular basis.
I have been able to use my nursing education and my knowledge of CRPS to help others. This was a win, win! My advice is to find something that you are passionate about. For some, that is art: painting, drawing or coloring. For others, their outlet is playing music. In addition to helping others, my pain distraction is crocheting. Whatever makes you happy and helps distract you from the pain is what you should be doing for yourself.
Another piece of advice is to learn everything that you can about CRPS. Read the literature. Watch YouTube videos. Talk to others with CRPS. Here are two YouTube Channels that I recommend. One is mine and the second that of Dr Pradeep Chopra. Dr Pradeep Chopra and Dr Ashraf Hanna are now considered the most experienced CRPS doctors.
If you are an audio learner, these YouTube channels will help you learn everything you need.
CRPS Insights
https://youtube.com/@crpscomplexregionalpains-qu3ww?feature=shared
Dr Chopra
https://youtu.be/S0FP6GidKwI?si=44hAxAbiKTyYg0-S
Dr Hanna
https://www.youtube.com/results?search_query=Dr+Ashraf+Hanna+MD+Clearwater
If you are a visual learner, I have an articles list on another page. Additionally, I have written three books that are sold on Amazon.
Books:
The Ketamine Handbook For CRPS
https://a.co/d/13eJVFa
CRPS and Alphabet Soup
https://a.co/d/4h4QZex
Children and CRPS: Children with Complex Regional Pain Syndrome and Associated Illnesses
Currently being updated.
Blogs:
https://crpstutor.blogspot.com/?m=1
http://nancyrsdcrpsblog.blogspot.com/2011/10/my-journey-through-crpsrsd-by-nancy.html?m=1
Facebook Support Groups that I administrate:
CRPS and Associated Illnesses: https://www.facebook.com/share/ZBKDM8RpQiPjTWhv/?mibextid=K35XfP
CRPS Newly Diagnosed: https://www.facebook.com/share/RUTo7rSnrXiTTgGo/?mibextid=K35XfP
CRPS Treatment Options https://www.facebook.com/share/Uh4N4uWA4H1LN5Xp/?mibextid=K35XfP
CRPS treatment using kethttps://www.facebook.com/share/g/1EW1x1SAAN/?mibextid=wwXIfr
FL CRPS Grouphttps://www.facebook.com/groups/761500759307816/?ref=share_group_link
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associated Illnesses: EDS
Ehlers-Danlos Syndrome - (EDS) is a group of inherited (passed from parent to child) connective tissue disorders. It is caused by mutations in genes encoding connective tissue proteins. The most prominent features are joint hyper-mobility, skin hyper extensibility, changes in the walls of the blood vessels and tissue fragility. This results in easy bruising and abnormal scarring. There are six major classifications of EDS. They are classic, hyper-mobility, vascular, kyphoscolitic, arthrochalasia and dermatosparaxis. The hyper-mobility type is the most common form of EDS followed by the classical type and vascular type.
Many children who develop CRPS have undiagnosed EDS.
EDS is a multisystem disorder.
EDS is a
- Chronic pain disorder
- Chronic fatigue disorder
- Gastrointestinal disorder
- Chronic headache disorder
- Causes pelvic dysfunction
- Causes cardio-vascular dysautonomia
- Causes immune dysregulation
In the case of someone with CRPS, it is repeated injuries caused by hyper-mobility of the joints that often causes the CRPS. Children who develop CRPS often have EDS as an underlying diagnosis. Joint hyper-mobility is determined by what is called the Beighton Scoring System. To be diagnosed with EDS hyper-mobility, you must have a score of four or more.
The Beighton score is calculated as follows:
1. One point if while standing forward bending you can place palms on the ground with legs straight
2. One point for each elbow that bends backwards
3. One point for each knee that bends backwards
4. One point for each thumb that touches the forearm when bent backwards
5. One point for each little finger that bends backwards beyond 90 degrees.








Associated Illnesses
Associated Illnesses: Dystonia
Dystonia - Many people also experience dystonia. Dystonia is defined as a neurological movement disorder, in which sustained muscle contractions cause twisting, repetitive movements or abnormal postures. Pain causes lack of motion and lack of motion leads to atrophy. Dystonia further adds to immobility and if not treated can be devastating to the person with CRPS causing them to be bedridden. I personally have dystonia. My toes curl, my calf muscle tightens, the muscles over my ribs tighten and my fingers curl. As my CRPS has progressed through the years, my dystonia has gotten worse. I know others who have rhythmic swallowing movements that are involuntary. Dystonia is a symptom of a larger category of symptoms called dysautonomia.



Dysautonomia
Dysautonomia- Dysautonomia is a disorder that disrupts your autonomic nervous system. The autonomic nervous system controls your blood pressure, heart rate, starting of movement, digestion, sexual arousal and breathing . You will see how this comes into play when we discuss how CRPS effects the body as a whole and causes associated syndromes.
Articles
Neridronate treatment for CRPS
Read More